
On this page we will be discussing checkpoint inhibitors and the main types that are currently being used in the treatment of some lymphomas.
What are checkpoint inhibitors?
Checkpoint inhibitors are medicines that block the signalling through immune checkpoints in a cell. Lymphoma cells can avoid detection by your immune system. Checkpoint inhibitors allow these checkpoints to be turned on and so lymphoma can be detected.
These checkpoints are a normal part of the immune system and keep immune responses from being too strong. By blocking them, these drugs allow immune cells to respond more strongly to cancer.
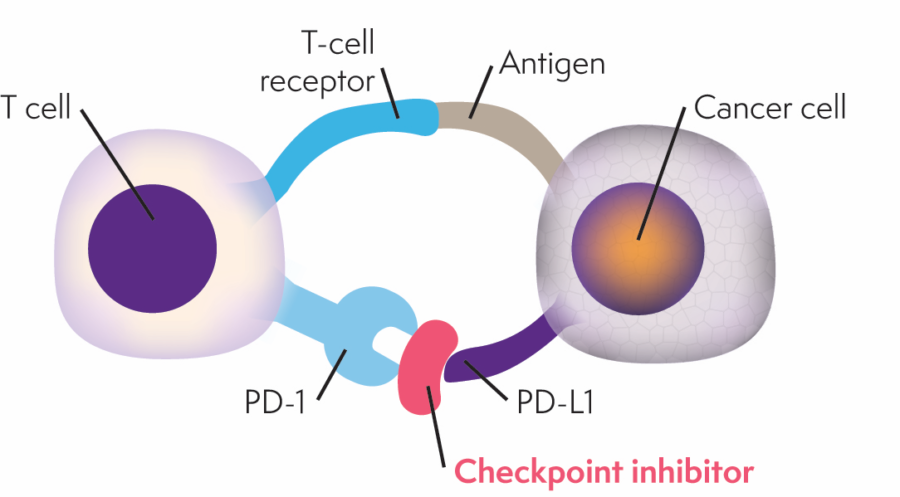
Our immune system’s T-cells have proteins on them that turn on an immune response and other proteins that turn it off. These are called checkpoints. Cancer cells sometimes find ways to use these checkpoints to hide from the immune system. They do this by making high levels of proteins to switch off T-cells when the T-cells should really be attacking the cancer cells.
Checkpoint inhibitors work by blocking the proteins that stop the immune system from killing cancer cells. When checkpoint inhibitors block these proteins, this turns the immune system back on and the T-cells can find and destroy the cancer cells. There are many different types of checkpoint inhibitors. Whether you have this treatment depends on what treatment you have had to date and the stage of your cancer.
Checkpoint inhibitors showing promise for lymphoma include:
- Pembrolizumab (Keytruda)
- Nivolumab (OPDIVO)
Pembrolizumab (Keytruda)
Pembrolizumab binds to PD-1 and blocks the checkpoint, allowing cancer cells that have PD-L1 to be destroyed by your immune system.
Indications of use in lymphoma
Pembrolizumab is currently publicly funded under the PBS for the following indications:
Classical Hodgkin lymphoma (cHL)
Monotherapy for the treatment of adult patients with relapsed or refractory classical Hodgkin Lymphoma (cHL):
- Following autologous stem cell transplant (ASCT) or
- Following at least two prior therapies when ASCT or multi-agent chemotherapy is not a treatment option.
Primary mediastinal B-cell lymphoma (PMBCL)
For the treatment of adult and paediatric patients with refractory primary mediastinal B-cell lymphoma (PMBCL), or who have relapsed after 2 or more prior lines of therapy.
How is it given?
- Given as an intravenous injection (into the vein)
- Given over 30 minutes
- Given every 21 days
- 35 cycles or until disease progression or unacceptable toxicity
Common side-effects
- Diarrhoea
- Nausea
- Joint pain
- Back pain
- Cough
- Fever
- Stomach pain
- Patches of skin which have
- lost colour
- Fatigue
- Decreased white cell count
Nivolumab (OPDIVO®)
Indications of use in lymphoma
Classical Hodgkin Lymphoma (cHL)
Used as a monotherapy. It is indicated for the treatment of patients with relapsed or refractory classical Hodgkin lymphoma (cHL) after autologous stem cell transplant and treatment with brentuximab vedotin.
How is it given?
It will be given to you as an infusion (a drip) into a vein (intravenously).
Administered intravenously over 30 minutes to 60 minutes
Your doctor will decide how many treatments you need.
Treatment should be continued if clinical benefit is observed or until treatment is no longer tolerated by the patient.
Possible side effects
- Infections of the upper respiratory tract
- Underactive thyroid gland, which can cause tiredness or weight gain
- Overactive thyroid gland, which can cause rapid heart rate, sweating and weight loss
- Decreased appetite
- Rash and itching
- Peripheral neuropathy
- Headaches
- Dizziness
- Inflammation of the lungs (pneumonitis)
- Inflammation of the intestines (colitis)
- Mouth ulcers and cold sores
- Pain in the muscles, bones, and joints
- Fever, oedema (swelling)
- High blood pressure



