

Overview of cutaneous (skin) lymphoma
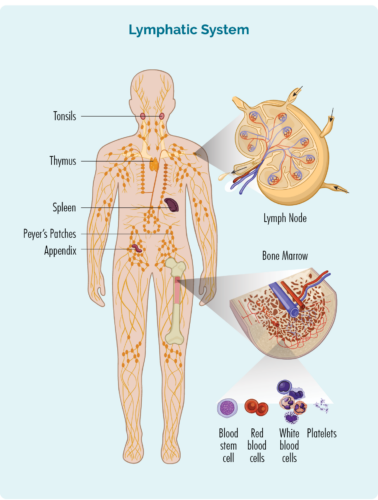
Lymphoma is a type of cancer that starts in white blood cells called lymphocytes. These blood cells usually live in our lymphatic system, but are able to travel to any part of our body. They are important cells of our immune system, fighting infection and disease, and helping other immune cells work more effectively.
About Lymphocytes
We have different types of lymphocytes, with the main groups being B-cell lymphocytes and T-cell lymphocytes. Both B and T-cell lymphocytes have a specialised function, having an “immunological memory”. This means that when we have an infection, disease, or if some of our cells are damaged (or mutated), our lymphocytes examine these cells and create specialised “memory B or T-cells”.
These memory cells keep all the information about how to fight the infection, or repair the damaged cells if the same infection or damage happens again. This way they can destroy or repair cells much faster and more effectively next time.
- B-cell lymphocytes also make antibodies (immunoglobulins) to help fight infections.
- T-cells help regulate our immune responses so that our immune system works effectively to fight infections, but also helps to stop the immune response once the infection is gone.
Lymphocytes can become cancerous lymphoma cells
Cutaneous lymphomas happen when either the B-cells or T-cells that travel to your skin become cancerous. The cancerous lymphoma cells then divide and grow uncontrollably, or do not die when they should.
Both adults and children can get cutaneous lymphomas and most people with cutaneous lymphoma will have cancerous T-cells. Only about 5 out of every 20 people with cutaneous lymphoma will have a B-cell lymphoma.
Cutaneous lymphomas are also divided into:
- Indolent – Indolent lymphomas are slow growing and often go through stages where they are “sleeping” causing no harm to you. You may not need any treatment if you have an indolent cutaneous lymphoma, though some people will. Most indolent lymphomas do not spread to other parts of your body, though some can cover different areas of skin. Over time, some indolent lymphomas can become advanced in stage, meaning they spread to other parts of your body, but this is rare with most cutaneous lymphomas.
- Aggressive – Aggressive lymphomas are fast-growing lymphomas that can develop quickly and spread to other parts of your body. If you have an aggressive cutaneous lymphoma, you will need to start treatment soon after you are diagnosed with the disease.
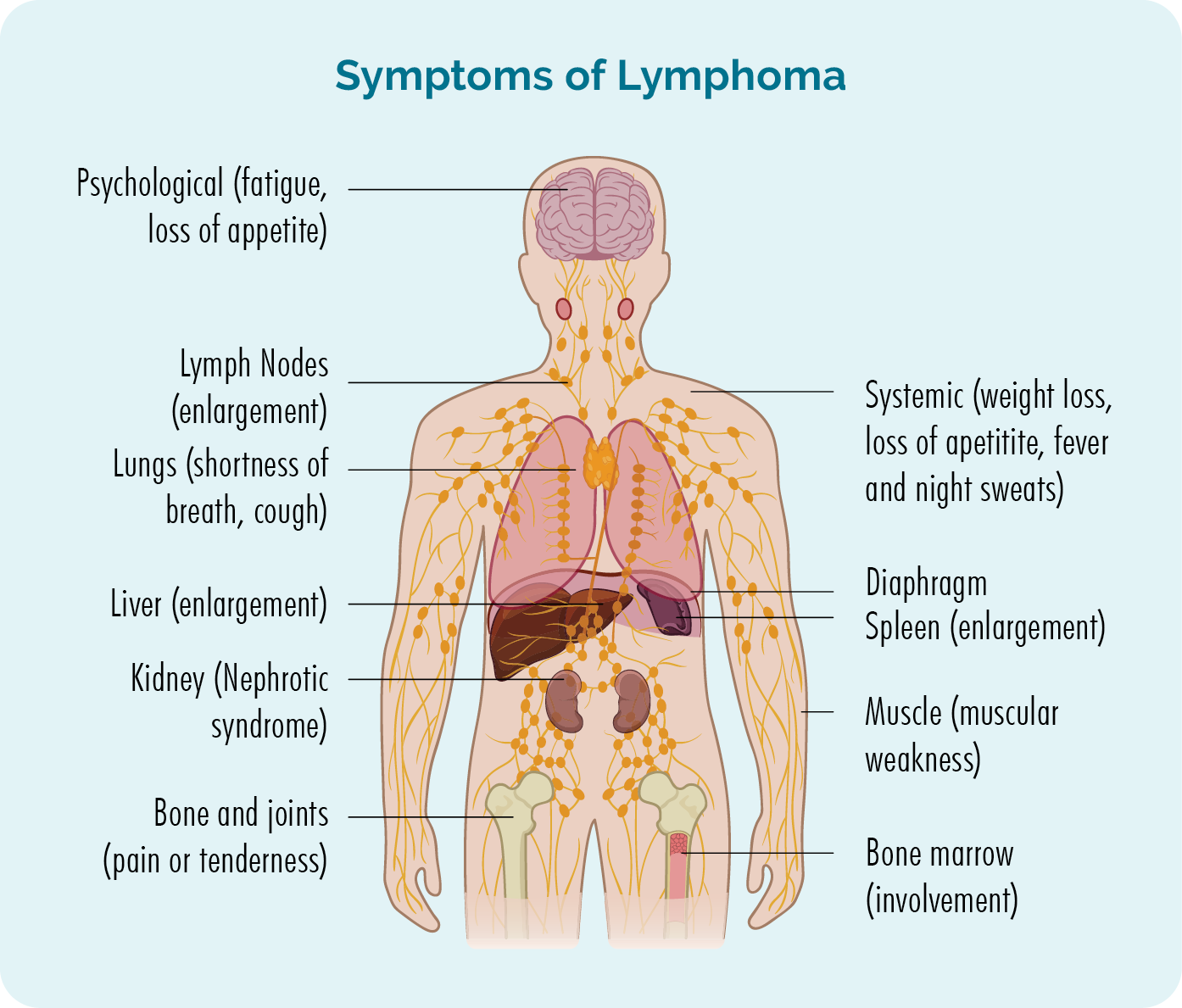
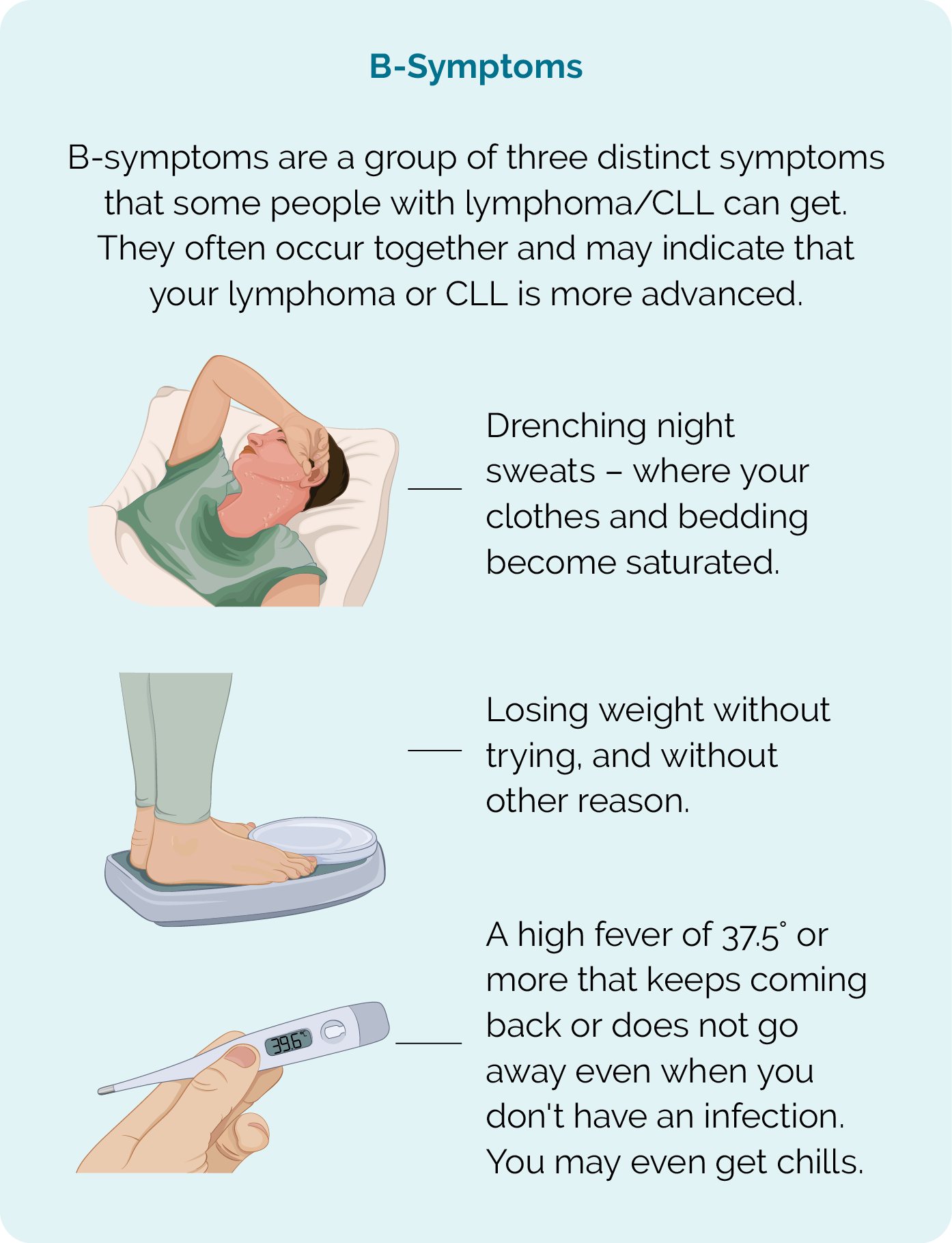
Symptoms of Cutaneous Lymphoma
Indolent cutaneous lymphoma
You may not have any noticeable symptoms if you have an indolent lymphoma. Because indolent lymphomas are slow growing, they develop over many years, so a rash or lesion on your skin may go unnoticed. If you do get symptoms they may include:
- a rash that does not go away
- itchy or painful areas on your skin
- flat, reddish, scaly patches of skin
- sores that can crack and bleed and not heal as expected
- generalised redness over large areas of skin
- a single, or multiple lumps on your skin
- If you have a darker colour skin, you may have areas of skin that are lighter than others (rather than redness).
You will need a biopsy or several biopsies to diagnose cutaneous lymphoma. The type of biopsy you have will depend on the type of rash or lesions you have, where they are located on your body and how big they are. It will also depend on whether it is only your skin that is affected, or if the lymphoma has spread to other parts of your body such as your lymph nodes, organs, blood or bone marrow. Some of the types of biopsies that may be recommended for you are listed below.
Skin biopsy
A skin biopsy is when a sample of your rash or lesion is removed and sent to pathology for testing. In some cases, if you have a single lesion, the entire lesion may be removed. There are different ways to perform the skin biopsy, and your doctor will be able to talk to you about the right skin biopsy for your circumstances.
Lymph node biopsy

If you have swollen lymph nodes that can be seen or felt, or that have shown up on scans, you may have a biopsy to see if the lymphoma has spread to your lymph nodes. There are two main types of lymph node biopsies used to diagnose lymphoma.
They include:
Core needle biopsy – where a needle is used to remove a sample of your affected lymph node. You will have a local anaesthetic to numb the area so you don’t feel pain during this procedure. In some cases, the doctor or radiologist may use an ultrasound to guide the needle into the right spot for the biopsy.
Excisional biopsy – with an excisional biopsy you will likely have a general anaesthetic so you sleep through the procedure. An entire lymph node or lesion is removed during and excisional biopsy so the entire node or lesion can be checked in pathology for signs of lymphoma. You will likely have a few stitches and a dressing when you wake up. Your nurse will be able to talk to you about how to care for the wound, and when/if you need to have the stitches removed.
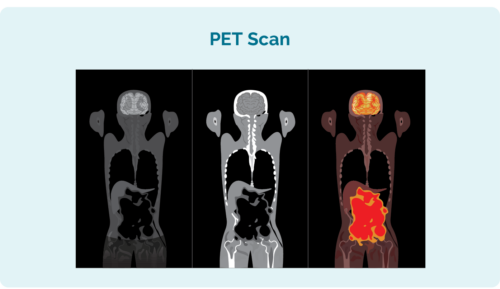 Positron Emission Tomography (PET) Scan
Positron Emission Tomography (PET) Scan
A PET scan is a scan of your entire body. It is done in a special section of the hospital called “nuclear medicine” and you will be given an injection of a radioactive medicine that any lymphoma cells absorb. When the scan is taken, the areas with lymphoma then light up on the scan to show where the lymphoma and the size and shape of it.
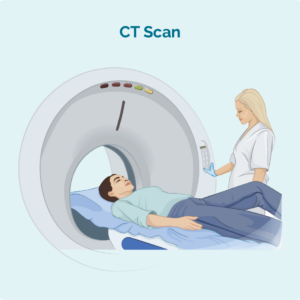
Computed Tomography (CT) scan
A CT scan is a specialised X-ray that takes 3 dimensional pictures of the inside of your body. It usually takes a scan of an area of your body such as your chest, abdomen or pelvis. These images can show if you have swollen lymph nodes deep inside your body, or areas that look cancerous in your organs.
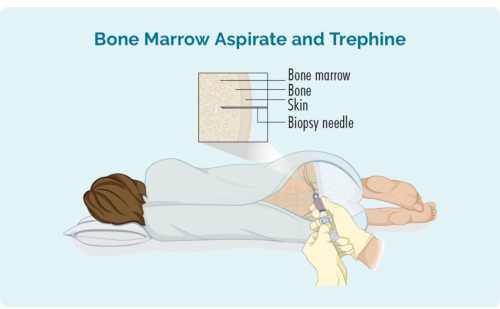
Bone Marrow Biopsy
Most people with cutaneous lymphoma will not need a bone marrow biopsy. However, if you have an aggressive subtype, you may need one to check if the lymphoma has spread to your bone marrow.
Two types of biopsies are taken during bone marrow biopsy:
- Bone marrow aspirate (BMA): this test takes a small amount of the liquid found in the bone marrow space
- Bone marrow aspirate trephine (BMAT): this test takes a small sample of the bone marrow tissue

{kind=link}
{kind=link}