
New treatments for lymphoma are changing how we treat lymphoma – a complex group of cancers. Two of the newest types of treatment are Bispecific Antibodies and Antibody Conjugates. Both of these treatments are advanced types of Monoclonal Antibodies (MABs).
MABs work by helping your own immune system find and destroy lymphoma cells more effectively.
Monoclonal Antibodies
What Does “Monoclonal” Mean?
The word monoclonal means made from one (mono) single type of cell which is then cloned (or duplicated) many times. Scientists make monoclonal antibodies (MABs) in a laboratory, so they are all the same, and target a specific antigen (a protein or receptor) on the lymphoma cells.
What Are Antibodies?
Antibodies are natural proteins made by our Plasma cells to fight infection. Plasma cells are specialised, mature B-cell lymphocytes – an important part of our immune system. Most of them are shaped a bit like the letter Y.
Each antibody locks onto a specific target called an antigen. All cells, good and bad, have different antigens on them. But each antibody can only recognise and lock on to one type of antigen. This helps the immune system recognise and destroy germs or diseased and damaged cells, or, recognise and protect healthy cells.
Scientists copy and genetically change antibodies – either from humans or animals, to make them target specific antigens to lymphoma cells. They then clone these antibodies so they can be used as medicine to fight diseases like lymphoma.

Rituximab
Rituximab is an example of a monoclonal antibody that has been used to fight lymphoma in Australia since 1998. Rituximab targets and locks on to an antigen called CD20.
It was first approved to treat people with Diffuse Large B-cell Lymphoma (DLBCL) and is still used today, not only to treat DLBCL, but for many subtypes of Non-Hodgkin Lymphoma that express the CD20 antigen.
Many people have a better chance of being cured or having long-term remission from lymphoma, because of rituximab.
Side-effects of MABSs
The below are common side-effects of all MABs. They are usually mild and temporary. However, if they concern you, talk to your doctor about how to best manage them.
- Fever and/or chills
- severe tiredness (fatigue}
- headache
- muscle aches or weakness
- rash or itching
- nausea
- diarrhoea
- low blood pressure during infusion
- infusion related reactions – these are usually mild and temporary and can occur while you are having the medicine or soon after. It can feel like any of the above symptoms. Your nurses will be ready to manage these symptoms very quickly if you have them.
Premedication such as paracetamol, antihistamine, or steroids are often given before you have a MAB treatment to reduce these effects.
Bispecific Antibodies & Antibody Conjugates
Although rituximab improved outcomes for many people with lymphoma, it did not cure everybody. So, researchers continue to look for new and better ways to treat lymphoma, or how they can improve current treatments. This is how the idea for bispecific antibodies and antibody conjugates were developed.
Both Bispecific Antibodies and Antibody Conjugates are laboratory-made monoclonal antibodies. But they include extra parts that help them work better against some lymphoma cells.
The next part of this webpage will discuss Bispecific Antibodies, followed by Antibody Conjugates. We will then discuss things to be aware of and consider before, during and after treatment with either of these treatments.
Bispecific Antibodies
How Bispecific Antibodies are made
To make Bispecific Antibodies, scientists join two different antibody parts into one molecule. One part of the antibody attaches to the lymphoma cell, and the other part attaches to a T-cell – a strong disease fighting immune cell.
By doing this, the Bispecific Antibody brings the T-cells straight to the lymphoma cell so it can destroy the lymphoma.

How Bispecific Antibodies Work
Bispecific Antibodies act as a bridge between your T-cells and the lymphoma cells. When the Bispecific Antibodies bind to both, it activates your T-cells.
Once activated, the T-cells release natural chemicals – called cytokines, that kill the lymphoma cell. These cytokines also help alert other cells of the immune system that there is work to be done to eliminate the lymphoma – helping to activate the rest of your immune system too.

Bispecific Antibodies available in Australia
- Epcoritamab (Epkinly®) is used for people with Relapsed or Refractory Diffuse Large B-cell Lymphoma (DLBCL).
- Blinatumomab (Blincyto®) is used for people with B-cell Acute Lymphoblastic Leukemia/Lymphoma (B-ALL).
Approved but not yet funded
Glofitamab (Columvi®) is another Bispecific Antibodies that is approved by the Therapeutic Goods Administration (TGA) in Australia. It can legally be used to treat people with relapsed or refractory DLBCL. However, it is not yet publicly funded (as of November 2025).
This means it may be expensive for you to access it. The manufacturer (Roche) is currently working with the Pharmaceutical Benefits Advisory Committee (PBAC) to get funding approved to make it cheaper to access.
Side-effects of Bispecific Antibodies
Common: Fever, chills, fatigue, rash, mild diarrhoea, low blood counts.
Less Common but Serious: Cytokine release syndrome (CRS), neurological effects, severe infection.
Side-effects from bispecific antibodies include the general side-effects we listed above. However, the release of lots of cytokines at once can sometimes cause more serious side-effects.
Cytokine Release Syndrome (CRS)
CRS is the most common and potentially serious side effect associated with Bispecific Antibody therapy. Cytokines are naturally occurring chemicals in our bodies that help our T cells to work. When you have a Bispecific Antibody treatment your immune system may produce more cytokines than usual.
This is a good thing as it helps your body fight the lymphoma. But it can sometimes also result in unwanted side effects. These may be mild flu-like symptoms or be more serious causing inflammation to all your body organs.
When does CRS happen?
CRS is most common during your first or second dose of a bispecific antibody when you have the more lymphoma in your body. These symptoms may start within hours of the medicine or occur weeks later.
If you get a temperature after the second round of bispecific antibody, you still need to go to the emergency department and call your haematologist. It may be something else called febrile neutropenia which also needs to be treated urgently.
Preventing CRS
CRS is more common in people with large amounts of lymphoma and who are having high doses of bispecific antibodies.
To prevent CRS happening, your haematologist may choose to use “step-up-dosing”. This is when you get a smaller dose of the bispecific antibody to start with. This is to limit how quickly the lymphoma breaks down. Then, as the lymphoma shrinks, they can give you more bispecific antibody with less risk of CRS.
Symptoms of CRS
CRS always causes a fever, and this is the defining symptom of CRS. If you don’t have a fever, you do not have CRS.
However, a fever can also be a symptom of infection (which also needs urgent treatment), so it is always important to go to the emergency department AND call your haematologist or specialist lymphoma nurse immediately if you get a fever after having a bispecific antibody.

If there is no one who can drive you immediately, call an ambulance on 000.
Other possible symptoms of CRS
If you do not have a fever, you do not have CRS. But if you do have CRS, you will have a fever, and may or may not have any of the below symptoms.
- low blood pressure
- low oxygen levels
- nausea, vomiting or loss of appetite – not wanting to eat
- difficulty swallowing
- extreme tiredness or fatigue not improved with sleep and rest
- shortness of breath and/or coughing
- dizziness
- confusion and/or hallucinations
- diarrhoea
- body aches and pains particularly in your muscles and joints
- rash
- swelling in your arms or legs.
Neurotoxicity (ICANS)
Neurotoxicity is another side effect of Bispecific Antibody therapy, which is caused from the release of lots of cytokines in a short time. Neurotoxicity associated with Bispecific Antibodies is often called Immune Associated Neurotoxicity Syndrome (ICANS).
Most people that get ICANS have also had Cytokine Release Syndrome (CRS), but rarely it can happen even if you haven’t had CRS.
ICANS can happen at any time, but usually starts soon after CRS, and within a month of having the treatment. It is very rare to get it after a month.
Symptoms of ICANS include:
- difficulty talking
- difficulty writing – or writing getting messier
- confusion, difficulty concentrating or feeling agitated.
Like CRS, ICANS can be mild or serious and needs treatment quickly. When treated, the symptoms are temporary and reversable, and you should have no lasting problems.
If you experience any of the above side effects, go to the emergency department and call your Haematologist or specialist lymphoma nurse immediately.
Both CRS and ICANS are most common on the first cycle of your Bispecific Antibody. The risk gets less each time as you have less lymphoma in your body. However, these side-effects can be serious and even life-threatening without quick treatment. You will be asked to stay in hospital, or close to the hospital for at least 24 hours (1 full day) after your first dose of a Bispecific Antibody.
Infection Risk
Infection is a common yet serious risk when you have treatment with a Bispecific Antibody. Your doctor may prescribe antibiotics and antiviral medicine that you take even if you don’t have infection. They are to prevent an infection and it is very important that you take them as they are prescribed.
Let your doctor or nurse know if you have any of the below symptoms:
- Fever (38°C or higher), with or without chills and shaking.
- Cough or shortness of breath.
- Tightness or pain in your chest.
- Flare up of sexually transmitted diseases or infections (STD’s or STI’s) such as herpes or warts.
- Flare up of cold sores, mouth sores or shingles.
- Feeling generally unwell.
- New rash.
Tumour Flare Reaction
Tumour Flare Reaction is a rare side-effect that can happen, usually after the first dose of a Bispecific Antibody. It is a temporary increase in the size of your lymphoma lesions/tumours. This can be concerning as it may look like the lymphoma is getting worse. But it is believed that tumour flare may happen because of the increase of immune cells infiltrating the tumour, and the inflammation process that happens as lymphoma cells break down, rather than the lymphoma getting worse.
Symptoms can include:
- pain
- redness or swelling.
- fever
In some cases, if your lymphoma is close to an important structure or organ, like your heart, lungs, airway or spine, your haematologist may want to shrink the tumour a bit before the treatment with a Bispecific Antibody. This is to avoid the risk of tumour flare causing pressure against these organs. This can be done with radiotherapy or other treatments.
Tumour Flare is usually easily treated with a type of medicine called corticosteroids (such as prednisolone, dexamethasone).
Antibody Conjugates
How Antibody Conjugates are Made
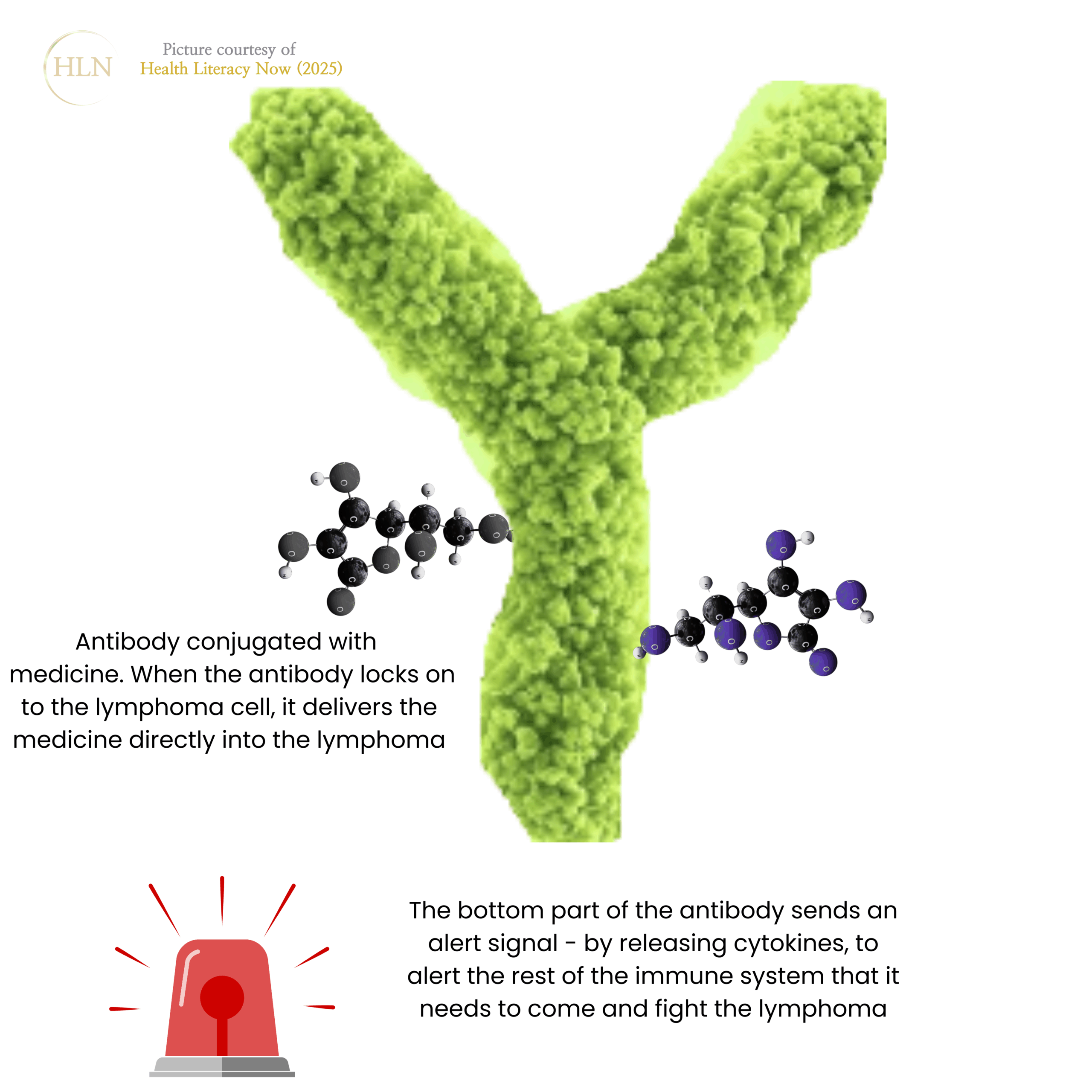
Antibody Conjugates are antibodies joined to another medicine such as a toxin, chemotherapy, or a radioactive particle. The antibody acts like a delivery vehicle, driving the attached medicine past your healthy cells and straight to the lymphoma cell.
This helps deliver the lymphoma fighting medicine straight to the lymphoma while protecting healthy cells.
* Antibody Conjugates are sometimes called Conjugated Antibodies
How Antibody Conjugates Work
Antibody Conjugates deliver the medicine or radiation straight into the lymphoma cell. The antibody seeks out and sticks to the targeted antigen on the lymphoma cell. Then, the attached medicine enters the lymphoma cell and destroys it from within.
Antibody Conjugates available in Australia
- Brentuximab vedotin (Adcetris®), used for people with CD30+ T-cell Lymphomas, or people with relapsed or refractory Hodgkin Lymphoma.
Approved but not yet funded
Polatuzumab vedotin (Polivy®) is approved by the TGA but not yet publicly funded, meaning it may be expensive to access. This Antibody Conjugate can be used for people with DLBCL who have:
- never had treatment. It is given with other medicines including a MAB (rituximab), chemotherapy (cyclophosphamide and doxorubicin) and a steroid (prednisone).
- relapsed or refractory DLBCL. It is given with rituximab and another chemotherapy called bendamustine.
Locastuximab tesirine-lpyl (Zynlonta®) has been registered for consideration with the TGA but is not available on the PBS. It may be available for some people on a compassionate access program for 3rd-line treatment if you have relapsed or refractory DLBCL (after you’ve already had 2 lots of treatment).
Side-effects of Antibody Conjugates
Common: Tiredness, nausea, diarrhoea, low blood counts, numbness or tingling in hands or feet (peripheral neuropathy).
Less Common but Serious:
- severe infection,
- liver, kidney, heart or lung changes,
- infusion related reactions,
- reactivation of Human Polyomavirus 2 (also called John Cunningham Virus – JCV),
- Tumour Lysis Syndrome (TLS).
If you have any signs of infection (listed above), let your doctor or nurse know immediately. You will have regular blood tests to check your liver and kidney function, and to test for Tumour lysis syndrome.
Tumour Lysis Syndrome (TLS)
TLS happens when you have a lot of lymphoma in your body. When the treatment begins to destroy the lymphoma cells, the waste products from destroyed cells spill into your blood. Adding to this, your own immune response can increase inflammatory proteins and cause changes in your blood tests.
TLS is a serious, but very treatable condition. You may need intravenous fluids or extra medicine temporarily to help control the TLS however, there should be no lasting effects if caught, and treated early.
Alternative access to medicine
There may be different treatments available, but not routinely available in Australia, or they are very expensive (such as Glofitamab® and Polatuzumab Vedotin® mentioned above). However, in some cases, there may be other ways to get these treatments.
Ask your doctor about alternative or compassionate access schemes and if these may by an option for you. Also see our YouTube video for more information TAKE CHARGE: Alternative access to medications not PBS listed. Presented by Prof Michael Dickinson
Safety Screening Before you start Bispecifics or Antibody Conjugates
Before starting, your doctor will organise several tests to make sure it is safe for you to have these treatments. These will include tests for:
- Hepatitis B and C – virus affecting your liver,
- Tuberculosis (TB) – a bacteria that can affect your lungs,
- How well your heart, liver, lungs and kidney are working,
- Pregnancy (for females of child baring age),
- Current medicines you take including prescribed medicines, supplements, over the counter and illicit drugs. It’s important to be honest about these. You will not get into trouble and will not be reported to police. But the doctor needs to know about them because they can affect how the treatment works.
- Any allergies you have or past infusion reactions.
They will also consider your lymphoma subtype, stage, other health conditions, and past treatments before deciding the best treatments options to offer you.
Other considerations and tests you may have
Vaccinations – Your doctor will ask you about your vaccinations. It is often recommended that you have vaccines like flu and COVID-19 boosters before starting. You will not be able to have live vaccines during and for some months after treatment. For more information on vaccines see our .
Blood tests – You will have blood tests before each treatment, and in some cases, in between doses. These blood tests check if your liver and kidneys are coping, and for TLS or other side-effects.
Infection Prevention – Wash your hands after going to the toilet, sneezing/coughing, touching food or common items such as trolleys, light switches and doorknobs. Avoid people with infections, or who have recently had a live vaccine.
Wash fruit and vegetables, eat freshly cooked food, avoid buffets, make sure food is in date. Only eat left-overs if they are less than 24 hours old and make sure you heat them thoroughly. If preparing food in advance – freeze it as soon as possible after cooking and only thaw when you are ready to eat it.
Ask your haematologist if you need antibiotic or antiviral medicine and take all medicines as they are prescribed.
Report any signs of infection to your doctor as soon as possible.
Fertility, Contraception and Breastfeeding – Do not get pregnant during treatment – some treatments can harm the unborn baby. Use barrier protection when having sex – like condoms or dams throughout the course of your treatment. Also talk to your doctor about the best type of contraception for you to use.
If you are planning to have a baby in the future, ask your doctor:
- What options are available to protect my fertility?
- How soon after treatment can I plan to get pregnant, or get my partner pregnant?
- Can I breastfeed?
If you are already pregnant see our webpage Pregnancy and Lymphoma
Scans and other tests – You may need scans to check how much lymphoma is left in your body, or other tests to check to make sure your body is coping with the treatment.
Rural and Remote Patients – Ask about telehealth appointments, accommodation & travel support, how long you will need to be away from home and local follow-up options. Also see our
Cultural and Language Access – You can ask for an interpreter or translated materials. Bring a support person if you wish.
During and after treatment
How Treatment Is Given and Monitored – Bispecific Antibodies and Conjugated MABs are given as injections under your skin, or as an infusion into your vein while you are in hospital or the treatment clinic. Before you have the treatment, you will have premedication to lessen the risk of having a reaction. After the premedication you may need to wait 30-60 minutes before you can have the treatment. This wait gives the premedication time to work.
Some Bispecific Antibodies use step-up dosing to reduce side-effects. This means you start with a lower dose, and it is gradually increased to prevent serious side-effects. You may need to stay overnight for early doses. Regular blood tests are needed to monitor your response.
Driving, Work, and Daily Life – Avoid driving or operating machinery if you are dizzy or tired after treatment. Plan time off work and ask about travel support if living remotely.
When to Call Your Doctor – Call or go to hospital if you have fever of 38°C or higher, shortness of breath, chest pain, confusion, seizures, yellowing of skin or your eyes, or tingling or weakness.
Side effects – We have listed the most common, and most serious side-effects earlier. However, this is not a comprehensive list. Talk to your doctor about the side effects, you should be aware of, how to recognise them, and when to let the doctor know about them. You can also see more information on managing side-effects at our website:
Clinical Trials and New Developments – Bispecific Antibodies and Conjugated MABs are being tested in more lymphoma types and earlier stages of lymphoma. You can search for current trials, here , or talk to your haematologist about clinical trials you may be eligible for. You can also give our nurses a call on 1800 952 081 – Monday – Friday 9am-4:30pm, AEST.
Important note and Questions to ask your Doctor
This webpage was written in November of 2025. New treatments may become available, or others may (rarely) stop being available. Additionally, depending on the individual bispecific antibody or antibody conjugate you have, you may have different side-effects from the ones listed. This factsheet does not replace medical advice. Always ask your doctor about:
- The best treatment option for you,
- The side-effects you need to report,
- When and how to report side-effects – including after hours
- Costs of treatment
- If there are any alternative access or compassionate access schemes you may be eligible for if you have relapsed or refractory lymphoma
- If there is a clinical trial you are eligible for.
Summary
- Bispecific antibodies (Bispecific Antibodies) and Conjugated MABs are newer targeted MABs that help your own immune system fight lymphoma more effectively.
- While they may reduce harm to healthy cells, they can still have serious side-effects – which can be treated. Report all side-effects to your treatment team as early as possible.
- Most serious symptoms from these treatments are a result of enhanced immune responses against the lymphoma, or the rapid destruction of lymphoma cells.
- Your team will monitor and manage side-effects. These treatments are improving outcomes and continue to be studied for future use.
- Ask about fertility preservation before starting treatment and when it would be safe to plan a pregnancy/breastfeeding.
- For a full list of side-effects talk to your haematologist/oncologist or pharmacist.
For a more comprehensive list of questions to ask your doctor, visit our and download the factsheets or call our nurses on 1800 953 081 to have a factsheet sent to you by post, with more questions to consider asking your doctor.