

To understand PCNSL you need to know a bit about your B-Cell lymphocytes.
B-Cell lymphocytes:
- Are a type of white blood cell
- Fight infection and diseases to keep you healthy.
- Remember infections you had in the past, so if you get the same infection again, your body’s immune system can fight it more effectively and quickly.
- Are made in your bone marrow (the spongy part in the middle of your bones), but usually live in your lymphatic system which includes your:
- lymph nodes
- lymphatic vessels and lymph fluid
- organs – spleen, thymus, tonsils, appendix
- lymphoid tissue
- Can travel through your lymphatic system, to any part of your body to fight infection or disease.

What happens when PCNSL develops?
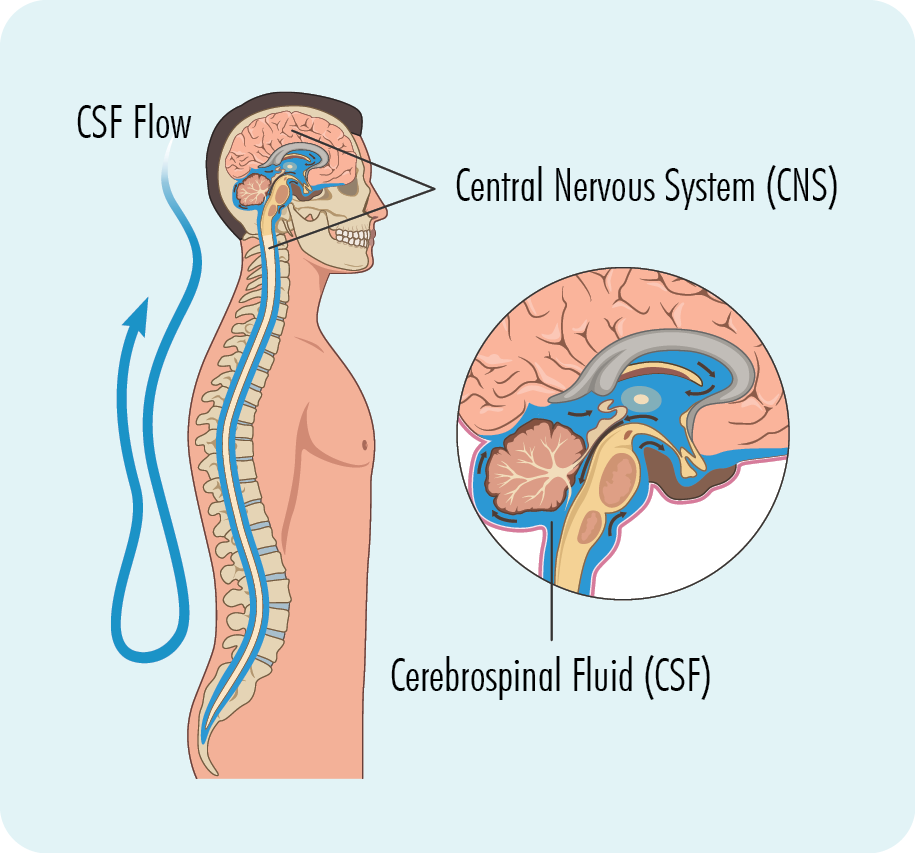
PCNSL develops when cancerous lymphocytes are found in your central nervous system (CNS), which includes your brain, spinal cord, eyes, cranial nerves and the protective layer of tissue that covers your brain and spinal cord called meninges.
When you have PCNSL, your cancerous lymphocytes:
- Grow uncontrollably
- Will not work as effectively to fight infections and disease
- Can become larger than they should and can look different to your healthy B-cells
- Can cause lymphoma to develop in your brain, spinal cord and eyes.
- Because of the protective barriers around our CNS, PCNSL does not usually spread to other parts of your body like other types of lymphoma can however, they can sometimes to spread the testes in males.
Biopsy
To diagnose PCNSL you will need a biopsy. A biopsy is a procedure to remove part, or all of an affected lymph node or affected tissue. During the procedure you may have either a general or local anaesthetic to make you more comfortable, or to ensure you are not awake while it is done.
The type of biopsy to be done will depend on where the lymphoma is located.
If the lymphoma is thought to be in your:
- Brain – a neurosurgeon (a specialist in diagnosing and treating problems with the CNS) takes a brain biopsy. Lumps (or samples of the lumps) within your brain will be removed using a CT scan to help guide the biopsy needle to the right area. This is called a ‘stereotactic biopsy’. You will have a general anaesthetic for this procedure as it is important not to move.
- Eye – an ophthalmologist (specialist in diseases and injuries of the eye) may take a little of the vitreous (gel-like substance inside your eye) to check for lymphoma cells.
- Spine – a specialist radiologist may take a biopsy from your spine.
Blood tests
Blood tests are also taken when trying to diagnose your lymphoma, but also throughout treatment so the doctor can get a better understanding of your overall health, and make sure your organs are working properly to cope with treatment.
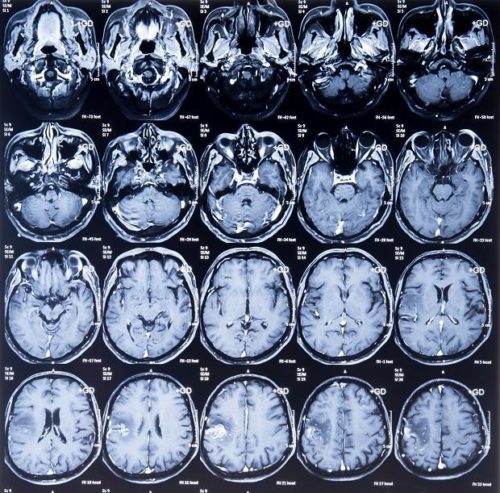
This scan usually gives the best images of your brain and other parts of the CNS and can also detect spinal cord compression.
These scans are usually done to detect lymphoma elsewhere in the body. They provide detailed pictures that provide more information than a standard X-ray. They may also be done to look at the bones on your spine.

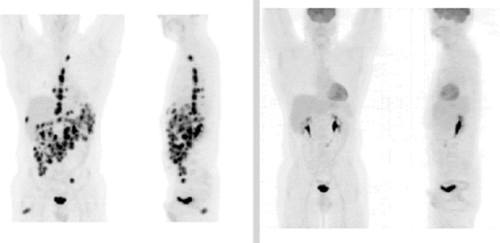
This type of scan is often used in combination with a CT scan to detect active lymphoma elsewhere in your body. It takes a picture of the inside of your whole body. You will be given a needle with some medicine that cancerous cells such as lymphoma cells, absorb. The medicine helps the PET scan to identify where the lymphoma is and the size and shape by highlighting areas with lymphoma cells. These are sometimes called “hot”.
As PCNSL can affect the eyes you may also need various ophthalmic tests. An ophthalmologist (eye specialist) will use an ophthalmoscope – an instrument with a light and small magnifying lens – to get a good look inside your eye. Certain imaging tests may be done and these help the ophthalmologist look at the tumour as well as see if the cancer has spread.
A biopsy of the eye may be needed. This is called a vitrectomy. A tiny instrument is inserted into the eye and it takes samples of the jelly-like vitreous, which is the substance that fills the middle of the eye.
A testicular ultrasound for men is a test that takes images of the testicles and the surrounding tissues in the scrotum.
This is done because some lymphomas start in the testes and spread to the central nervous system (CNS). If the lymphoma is found in your testes, then it is most likely that your CNS lymphoma is secondary rather than primary, and will therefore need different treatment.
Most testicular lymphomas are a subtype of Diffuse Large B-cell Lymphoma (DLBCL), but some are a subtype of Burkitt’s lymphoma, Mantle Cell Lymphoma (MCL), Follicular Lymphoma, or T-cell lymphoma.
Click on the links below to find more information on these subtypes.


