

Understanding NK and T-cell Lymphocytes
Lymphocytes are an important part of our immune system that protect us against infection and disease, and regulate our immune system to prevent autoimmune attacks. Auto immune attacks happen when our immune system is overactive or faulty and begins to fight our own body instead of infection and disease.
About Natural Killer (NK) cells and T-cell Lymphocytes
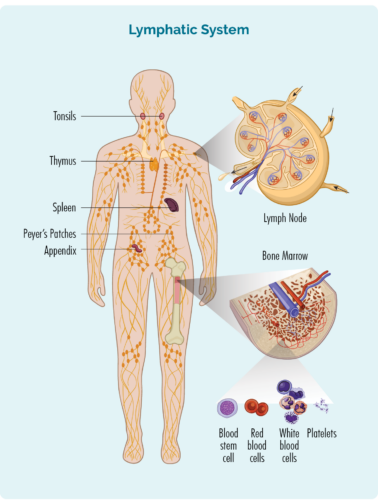
- T-cells are made in our bone marrow, mature in our thymus, but can live in any part of our lymphatic system – including our lymph nodes.
- Most T-cells need to be activated to work effectively. They are usually resting in our thymus or other parts of our lymphatic system, and only wake up and fight infection when other immune cells let them know there is an infection or disease to fight. When they wake up, T-cells can travel to any part of our body to fight the infection or disease.
- Some T-cells are responsible for “regulating” the immune response. This means that once an infection has been destroyed, the Regulatory T-cells tell other immune cells to “stand down” so they don’t keep fighting and cause harm to our good cells.
- Natural Killer (NK) cells are often called “NK T-cells”. They are specialised immune cells that recognise and destroy germs and cancer cells. Unlike other T-cells, NK cells do not need to be activated to fight cancer. They are ready to fight at all times, and actively move around your body on the look-out for cells that have cancerous changes.
- After fighting an infection or disease, some T-cells become “Memory cells”. They remember everything there is to know about the infection and how to fight it. That way, if we ever get the same infection or disease again, our immune system can fight it a lot more quickly and effectively.
- Some T-cells help other immune cells, such as B-cell lymphocytes to work effectively. These T-cells are called “Helper T-cells”.
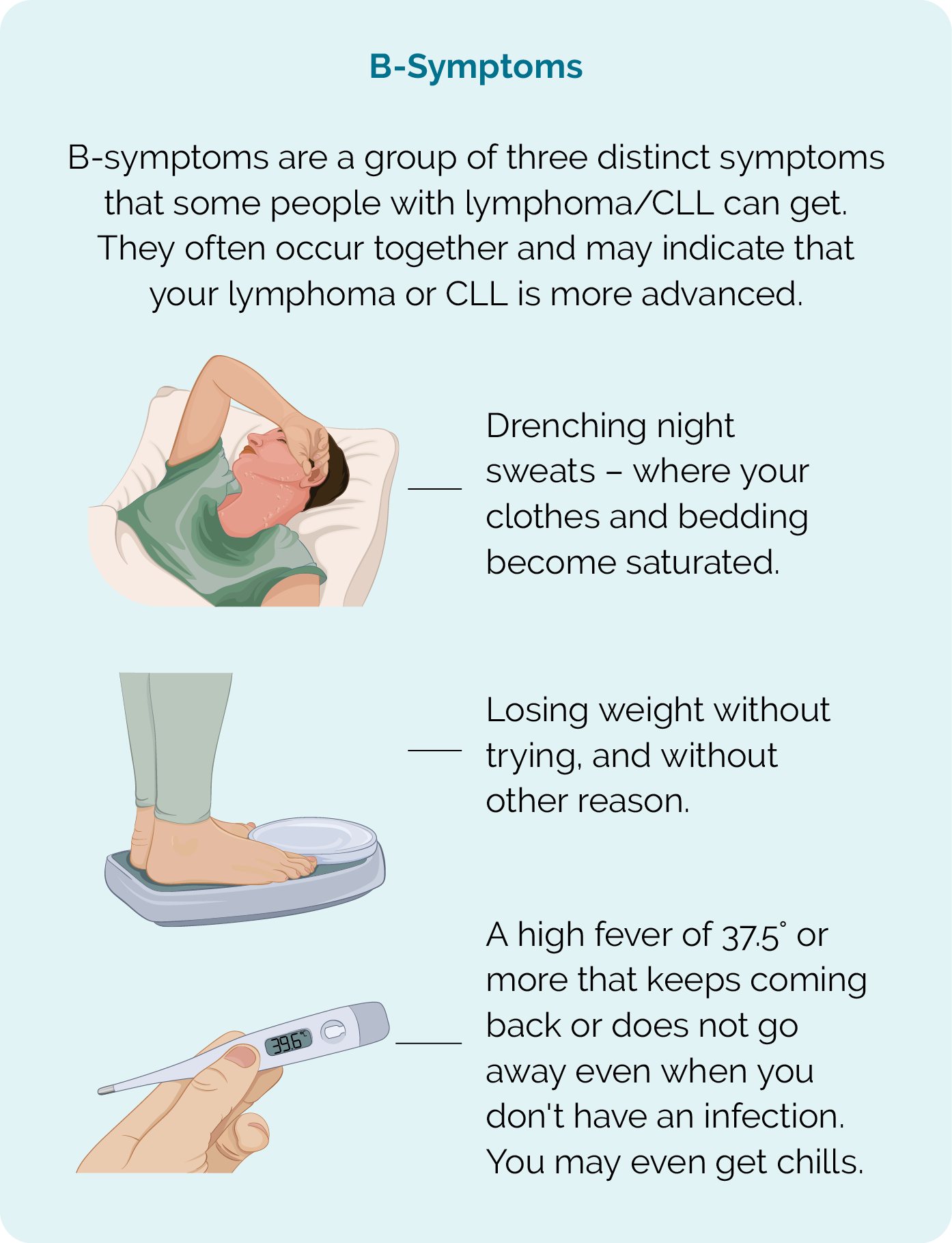
General symptoms of lymphoma
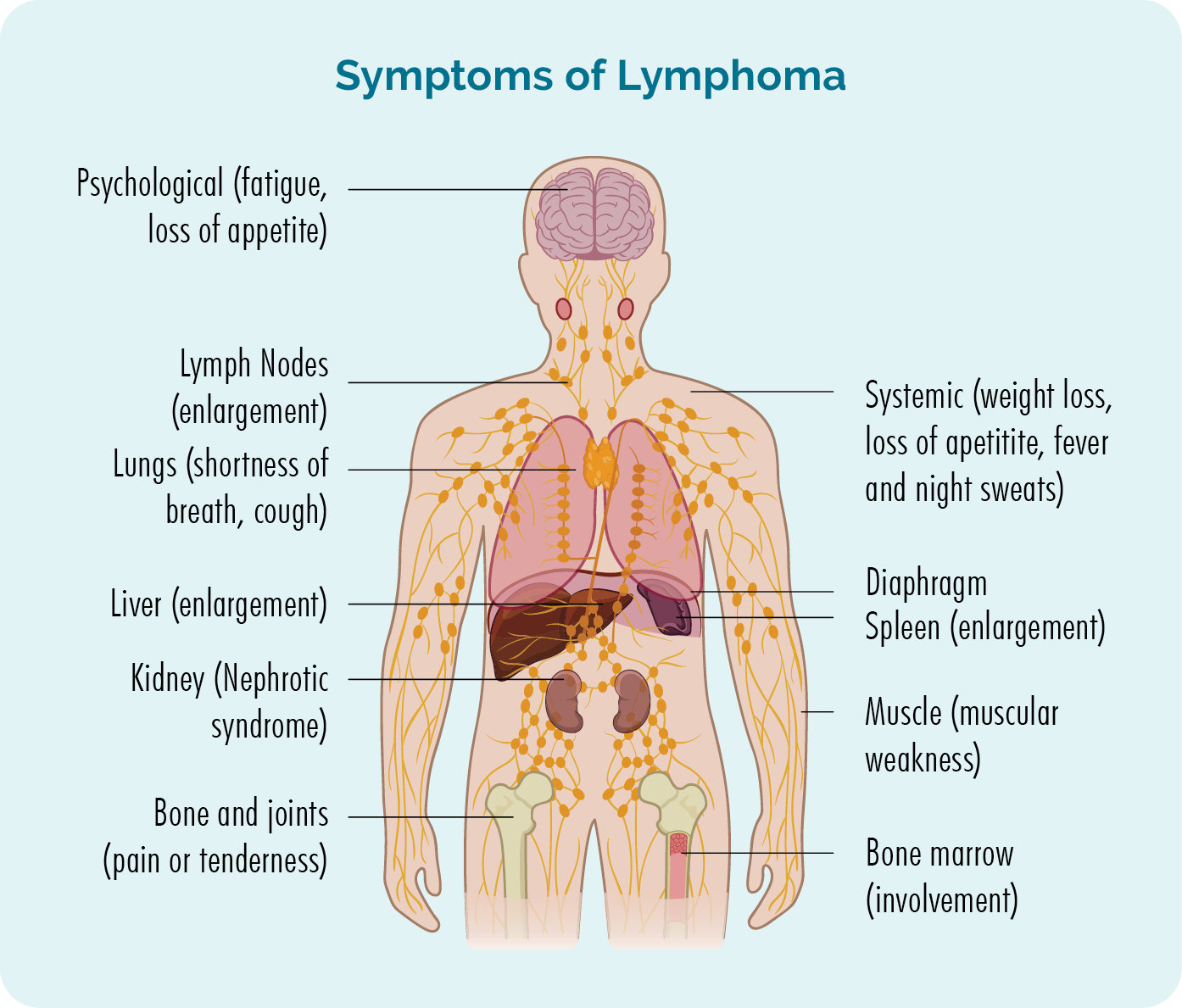
There are some symptoms that are common in many people with lymphoma, and others called B-symptoms that you need to report to your doctor quickly. These symptoms are shown in the pictures, but for an in-depth look at symptoms click on the link above.
Chemotherapy is a term used to describe many different medications that destroy fast-growing cells. Because they destroy fast-growing cells they are effective at treating many types of cancer, including Natural Killer T-cell Lymphoma.
Common Side-effects
Chemotherapy medications cannot tell the difference between healthy and cancerous cells. They only see that they are fast-growing. This means some of your good healthy cells can also be attacked by chemotherapy resulting in unwanted side effects such as:
- mouth sores
- nausea and vomiting
- diarrhea or constipation
- hair loss
- dry skin
- a drop in healthy blood cells
- fatigue – extreme tiredness not improved with rest or sleep.
Healthy cells are able to repair and reproduce more healthy cells quicker than cancerous cells, so you will have chemotherapy in “cycles”. You will have a round of chemotherapy, then a break while your healthy cells recover, and then another cycle. How many cycles you have and the break in between will depend on the treatment you get and your individual circumstances.
Chemotherapy protocols for NKTL
Some of the common chemotherapy protocols used to treat NKTL include:
- SMILE – Steroid [dexamethasome] Methotexate, Ifosphamide, L-asparaginase, Etoposide. You will also have supportive medications to help prevent side -effects and complications. These will include:
- calcium folinate to prevent toxicity from methotrexate
- mesna to protect your bladder from the ifosphamide
- GCSF to help your white blood cells recover.
Monoclonal antibodies (MABs) are medications that engage your immune system to help it fight the lymphoma more effectively.
There are different types of MABs and they work by sticking to a protein on your lymphoma cell. The MAB then sets off signals that alert your immune system to the threat of a lymphoma cell so your immune system can mount an attack and destroy the lymphoma.
In some cases, lymphoma cells can have a protein on them (PD-L1) that tricks your immune system into thinking it is a healthy cell. When the MAB attaches to these proteins it strips the lymphoma cell of its “mask” so your immune system can see it as a lymphoma cell. These MABs are called immune checkpoint inhibitors.
Other MABs are made with a medication toxic to lymphoma cells attached to them. They then seek out the protein (such as CD30 or CD38) on the lymphoma cell and stick to it. By sticking to lymphoma cell, these MABs deliver the toxic medication straight into the lymphoma cell to destroy it. These MABs are called conjugated MABs.
Some monoclonal antibodies that may be used to treat NKTL include:
- pembrolizumab, nivolumab (immune checkpoint inhibitor)
- brentuximab vedotin (conjugated MAB)

Radiotherapy uses high-energy x-rays (radiation), to kill cancer cells. It can be used as a treatment on its own, or with other treatments such as chemotherapy.
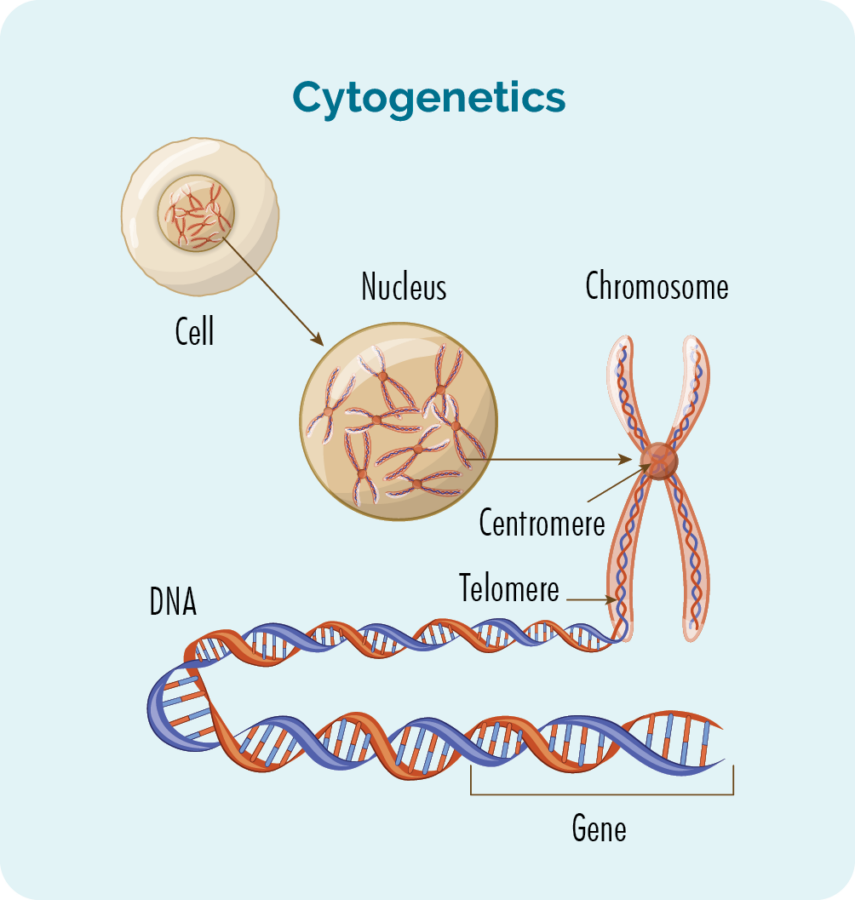
The X-rays cause damage to the cell’s DNA (the genetic material of the cell) which makes it impossible for the lymphoma to repair itself. This causes the cell to die. It usually takes a few days or even weeks after radiation treatment begins for the cells to die. This affect can last for several months though, so even months after you finish treatment, the cancerous lymphoma cells can still be destroyed.
If your NKTL is diagnosed in the early stages of disease, this may be the only treatment you need. However, it is also often given along with chemotherapy.
A stem cell transplant is a procedure that may be used to treat your lymphoma, or to keep you in remission for longer if there is high chance your lymphoma will relapse. Your doctor may also recommend a stem cell transplant for you when your lymphoma relapses.
A stem cell transplant is a complicated and invasive procedure that occurs in stages. Patients undergoing a stem cell transplant are first prepared with chemotherapy alone or in combination with radiotherapy. The chemotherapy treatment used in stem cell transplants is given at higher doses than usual. The choice of chemotherapy given in this stage depends on the type and intent of the transplant.
More information on Stem Cell Transplants
For more information on stem cell transplants see our following webpages.
Stem cell transplants – an overview
Autologous stem cell transplants – using your own stem cells
Allogeneic stem cell transplants – using somebody else’s (a donor’s) stem cells
Clinical trials are an important way of finding new and better ways to treat lymphoma. We always recommend asking your doctor about any clinical trials you may be eligible. Especially when you have a rare cancer such as NKTL, it offers extra opportunities to try different treatments that would otherwise not be available to you.
There are no guarantees with clinical trials, as their purpose is to test new medications or combinations of treatments to see if they work better than the current treatments.
Talk to you doctor about clinical trials if you are interested in participating in one.



